If you have diabetes, your body cannot use and store sugar properly. High blood sugar levels create changes in the veins, arteries, and capillaries that carry blood throughout the body. This includes the tiny blood vessels in the retina, the light-sensitive nerve layer that lines the back of the eye. The damage to retinal vessels is referred to as diabetic retinopathy.
With today’s improved methods of diagnosis and treatment of retinopathy, serious vision problems are largely preventable. Early detection of diabetic retinopathy is the best protection against loss of vision. You can significantly lower your risk by maintaining strict control of your blood sugar and visiting your ophthalmologist at least once a year. Work with your diabetes doctor (endocrinologist) to manage related issues like high blood pressure or kidney complications.
Types of Diabetic Retinopathy
Nonproliferative Diabetic Retinopathy (NPDR)
“Background Retinopathy”
Early stage of diabetic retinopathy
Blood or fluid leakage in the retina causes swelling or deposits of protein/cellular debris
NPDR has little effect on vision*
*Vision loss in NPDR cases is typically related to macular edema and/or macular ischemia
New blood vessels are grown in response, often accompanied by scar tissue that may cause wrinkling or detachment of the retina
May cause severe vision loss because it can influence both central and peripheral vision*
*Because PDR often has no early symptoms, if you have any form of diabetes, you should have your eyes examined at least annually by an eye M.D. (ophthalmologist)
Diagnosis and Treatment
A medical eye examination is the only way to find changes inside your eye. An ophthalmologist can diagnose and treat serious retinopathy before you are even aware of any vision problems. The standard of care for treating many of the complications of diabetic retinopathy is rapidly evolving. Severe vision loss is preventable in the vast majority of cases, and can possibly be improved.
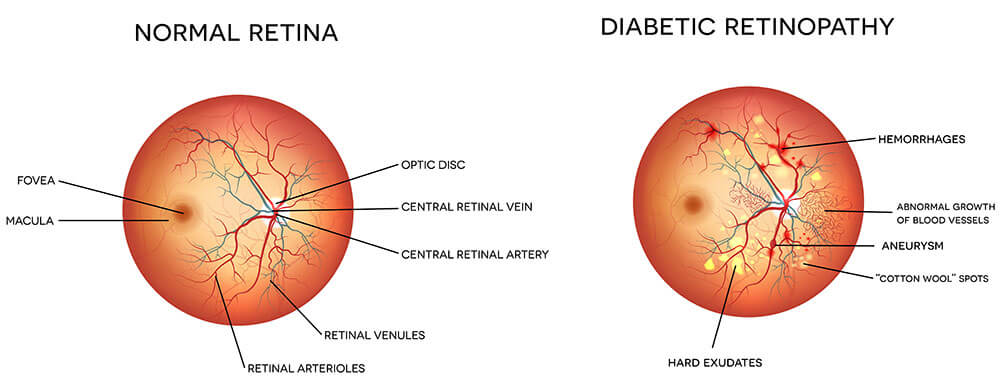
Normal eye retina compared to one affected by diabetic retinopathy.
Intravitreal Injection
Injections of potent medications in the eye are now commonly done in the office, and the results are usually very good. The injections are done with a local anesthetic, and can be done very rapidly (usually less than a few seconds for the actual injection). There is only a minimal amount of discomfort during and after the procedure. There are risks associated with the injections, just as there are with any surgical procedure, but these are very rare.
Laser Surgery
The main goal of laser treatment is to prevent further loss of vision. In a sense, it “freezes” the symptoms and keeps them from getting worse. Many people experience improvement; however, in most cases, “perfect” vision will not be completely recovered after laser treatment. Multiple laser treatments over time are sometimes necessary. Laser surgery does not cure diabetic retinopathy and does not always prevent further loss of vision.
For PDR, the laser is focused on all parts of the retina except the macula. This treatment (also known as panretinal photocoagulation) causes the abnormal new vessels to shrink and often keeps them from growing. It also decreases the chance that vitreous bleeding or retinal distortion will occur.
For macular edema, the laser is focused on the damaged retina near the macula to decrease the fluid leakage. People may rarely see the laser spots near the center of their vision following treatment, but these typically fade over the course of a few weeks.
Vitrectomy Surgery
In advanced PDR, the ophthalmologist may recommend a microsurgical procedure known as vitrectomy. During this procedure, which is performed in the operating room, the blood-filled vitreous is removed and replaced with a clear solution. The ophthalmologist may wait for several months or up to a year to see if the blood clears on its own before performing a vitrectomy. Surgery should usually be done early because macular distortion or traction retinal detachment will cause permanent vision loss. The longer the macula is distorted or out of place, the more serious the vision loss will be.